Scotland’s heroin deaths in decline
Last week came welcome news that deaths in Scotland in which heroin is implicated had dropped by 20 per cent from 322 in 2009 to 254 in 2010. The figures for England and Wales will be released later this month: will they also suggest a major decrease in heroin-related deaths?
And shall we have failure of the opium crop in Afghanistan to thank, or other reasons? The Highland Council will hope that Inverness’s promotion of take-home Naloxone (heroin antidote) may have contributed to its DRDs having reduced from 14 in 2009 to six in 2010 – but it’s too soon to tell.
Total drug-related deaths (DRDs) in Scotland in 2010 were 485, against 545 in 2009 and 574 in 2008. When last estimated (in 2006), Scotland had around 27,000 current injectors. Their annual heroin-related death-rate is as high as the death-rate of British soldiers in Afghanistan in 2011 - about 6 deaths per 1,000 person-years, and injectors’ death-rates may increase as they age.
The Table summarises Scotland’s DRDs by age-group for three 5-year epochs. Epoch 1 is 1996-2000; Epoch 2 is 2001-2005; and Epoch 3 is the newly-available 2006-2010.
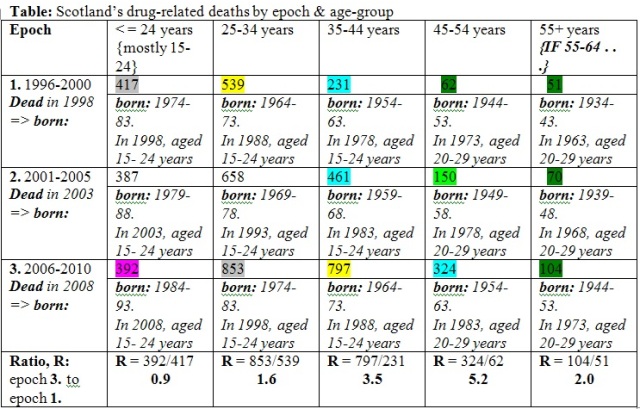
First, notice that the ratio of DRDs in Epoch 3 to Epoch 1, which is given in the bottom row of the Table, is very different by age-group: the ratio is around 1 for the youngest age-group but 3.5 and 5.2 for those who succumbed to DRD when aged 35-44 or 45-54.
The ratio of around 1 for the youngest age-group is because DRDs have taken the same toll of under 25s in each of the three 5-year epochs: around 400 DRDs. This should be interpreted as some measure of public health success: in the 1990s, Scotland has either capped its injector epidemic (which took off dramatically in the early 1980s) and may even have reduced it. Alternatively, if incidence has remained unchanged or has even increased, then the death rate per injector has been reduced. Whatever the explanation, there has been some success.
But how did the other ratios come about, and why are they so high?
For ease of interpretation, I’ll characterise each Epoch by the birth-cohort (born:) for a person who died mid-Epoch (that is: in 1998 for Epoch 1, 2003 for Epoch 2 or 2008 for Epoch 3).
For each mid-Epoch birth-cohort, I document their age-range in key calendar years (chosen from 1963 to 2008). Key calendar year increases by 5-years from one Epoch to the next as you read down any column in the Table.
Key calendar years, at 5-year intervals, have been chosen to span the period during which initiations to injecting drug use increased dramatically in Scotland (particularly between 1973 and 1988) and overlap between the bottom of one column and the top of the next as you read the Table from oldest DRD column (on the right) to youngest (on the left). The overlap gives assurance that the features of interest apply at more than one age-range.
Age-ranges were chosen to be 20-29 years or 15-24 years to reflect the ages at which initiations to injection drug use predominate.
And so, for each column in the Table (from right to left), key calendar years for the mid-Epoch birth-cohort were selected as follows, when their age-range was as specified:
Key calendar years are 1963, 1968, 1973 for those aged 55+ at DRD when successive mid-Epoch birth-cohorts are aged 20-29 years
Key calendar years are 1973, 1978, 1983 (for those aged 45-54 years at DRD) when successive mid-Epoch birth-cohorts are aged 20-29 years;
Key calendar years are 1978, 1983, 1988 (for those aged 35-44 years at DRD) when successive mid-Epoch birth-cohorts are aged 15-24 years
Key calendar years are 1988, 1993, 2003 (for those aged 25-34 years at DRD) when successive mid-Epoch birth-cohorts are aged 15-24 years
Key calendar years are 1993, 2003, 2008 (for those aged 15-24 years at DRD) when successive mid-Epoch birth-cohorts are aged 15-24 years.
We can now answer how the other ratios came about, and why they are so high. DRDs at 55+ years increased from 51 in 1996-2000 (the corresponding mid-Epoch cohort was born in 1934-43 and aged 20-29 years in 1963) to 70 in 2001-2005 and 104 in 2006-2010 (the corresponding mid-Epoch cohort was born in 1944-53 and aged 20-29 years in 1973). Scotland’s oldest-age DRDs increased by a factor of 1.4 between Epochs for which the mid-Epoch birth-cohorts were aged 20-29 years in 1963, 1968 and 1973 respectively. Other things being equal (quite a major assumption), we may assume that the incidence of heroin injecting had roughly doubled between 1963 and 1973.
Let’s now consider DRDs at 45-54 years of age which more than doubled between epochs: from 62 in Epoch 1 through 150 in Epoch 2 to 324 in Epoch 3. The corresponding mid-Epoch cohorts were aged 20-29 years in 1973, 1978 and 1983. Other things being equal (quite a major assumption), we may assume that the incidence of heroin injecting had increased by a factor of 5 between 1973 and 1983.
What insights do we glean from DRDs at 35-44 years of age which doubled in number from 231 to 461 between Epochs 1 and 2 (when the respective mid-Epoch birth-cohorts were aged 15-24 years in 1978 and 1983 respectively)? Thus, we have confirmation from the middle column of our Table of the above finding (based on DRDs at 45-54 years) that injector incidence appears to have doubled between 1978 and 1983. However, DRDs at 35-44 years of age reveal that incidence may have slowed between 1983 and 1988 when DRDs at 35-44 years increased by a factor of 1.7 from 461 in Epochs 2 to 797 in Epoch 3.
We use DRDs at 25-34 years of age to give hindsight to how initiations into injecting/problem drug use may have altered from 1988 to 1998. Since DRDs at 25-34 years of age increased only gradually by a factor of 1.3 or less between epochs – namely from 539 in Epoch 1 through 658 in Epoch 2 to 853 in Epoch 3 - it appears that, if other things remained equal (such as DRD-rate per 100 injectors), injector incidence may have slowed again during 1988 to 1998.
The leftmost column of the Table is used to infer what may have occurred in respect of injector incidence over the period 1998 to 2008. From the stable number of DRDs in the youngest age-group, we may hope that injector incidence has stabilized from 1998. However, it is too early to know if any important decrease in initiations has taken place.
I emphasis that ‘other things being equal’ is a major assumption. If, as is likely, injectors’ DRD-rate has decreased in the 21st century on account of greater uptake of opiate substitution therapy, then lower DRD-rate would mean that there could have been off-setting increases in injector incidence for the observed patterns to hold.
More sophisticated back-calculation is required to take competing factors into account. However, it remains encouraging that Scotland’s DRDs in the youngest age-group have not increased in the period 1996-2010. Scotland’s deputy Tory leader, Murdo Fraser, and The Scotsman (10 August 2011) would do well to turn their attention to how they/we can better support current injectors in their efforts not to initiate novices into heroin injecting.
That would better serve the public health than casting doubt on methadone therapy without which the lethal toll of heroin injecting would be graver still. Recovery, besides benefiting the individual, has the added benefit of reducing the pool of initiators. Methadone clients could, for example, be encouraged to discourage the initiation of novice injectors.
Murdo Fraser and the Scotsman were concerned that Scotland’s number of methadone-implicated DRDs had not decreased (169 in 2008, 173 in 2009 and 174 in 2010). As Strang et al. have shown, the number of methadone-implicated DRDs should be related to the volume of methadone prescribed when making comparison between calendar years, regions or nations.
Secondly, as Dr Robertson, chair of Scotland’s National Forum on Drugs-Related Deaths, has pointed out, the majority of methadone-implicated deaths occurs in those for whom methadone was not prescribed. Understanding of the risk factors involved would be well-served if a randomly sampled one in four methadone-related DRDs was made subject to Fatal Accident Inquiry (FAI) on which sheriffs made a written determination that was posted on the Scottish courts’ web-site.
Indeed, DRDs claim so many young lives that a random one in four of all DRDs might usefully be made subject to FAI by which sheriffs might tease out novel insights.
