Legal highs: catching up with new epidemics
Mephedrone, a designer drug, is a "legal high" that can be purchased via the internet, and has euphoric effects akin to cocaine or ecstasy, both of which are class A drugs.
There are indications that mephedrone use is rising quickly, possibly displacing cocaine for some drug-users. If this is indeed happening, there are potential implications for the numbers of drug-related deaths. But just what those implications may be is unknown because we lack data on mephedrone use, potential for dependency, and lethality.
These could be very different from those of ecstasy or cocaine. Per annum, ecstasy-related deaths were roughly 1 per 10,000 past-year users in 2004-2007 (95% CI: 0.8 to 1.2) whereas the cocaine-related death-rate in England and Wales was higher at around 2 per 10,000 past-year users. Cocaine-related death rate increases steeply with users’ age-group, notably by 5-fold when comparing 16-24 year olds versus 35+ year olds, and is disproportionately high for male users.
Applying prevalences estimated by the British Crime Survey (BCS) to the mid-2007 population of England and Wales, the number of 16-59 year old ‘past year users’ of cocaine approximated 800,000 to 1 million in 2007 – and greatly exceeded past-year users of ecstasy. In fact, past-year use of ecstasy in England and Wales was very significantly lower, by a fifth, at 1.67% (se 0.05%) during the most recent four BCS waves (2004-07) than in the previous three (2001-03).
The British Army conducts compulsory drug tests on soldiers on Mondays, in order to discourage the weekend use of drugs. The tests show that cocaine use apparently decreased quite markedly in 2009 from its previous level of around 9 cocaine-positives per 1,000 privates urine-tested on a Monday, see Bird et al. (2008)*. How dramatic is the decrease; and have privates substituted use of the “legal high”, mephedrone, for cocaine?
The army conducts around 24,000 Monday tests on privates per annum, and so about 6,000 in three months. On the results for previous years, we’d expect 54 cocaine-positives in that period. If a third of these had been displaced by a switch to legal mephedrone, then anonymised testing of all 6,000 samples taken in a three-month period might find 18 samples positive for mephedrone. Carrying out the tests could cost around £200,000, but it would give a hugely valuable up-to-the-minute insight into privates’ relative use at weekends of cocaine, ecstasy and mephedrone.
Two wider questions are:
- might privates’ altered recreational drug use presage a more general, major shift away from use of cocaine and its associated lethality?
- what do we know anyway about the lethality of mephedrone?
We don’t yet routinely test for mephedrone at UK’s drugs-related deaths, and so we cannot know how many of them had recently taken mephedrone, or had it present in such quantity as may have contributed to death.
Uptake of a ‘legal high’ with low to negligible lethality could be substantial. For example, use of cannabis use, although illegal, is highly prevalent. The lethality of mephedrone is currently unknown because, at present, UK does not routinely test all drugs-related deaths for mephedrone. How prevalent is past-year use of mephedrone?
According to Mixmag’s self-selected rave-scene respondents, use of mephedrone has quickly risen to about two-thirds the prevalence of cocaine use. The extent to which this ‘legal high’ has displaced the use of cocaine (as may be the case among army privates) or has attracted new users who hitherto avoided cocaine because of its dependency, lethality, classification and illegality is unclear – pending data from BCS in autumn 2010.
Rapid rise in prevalent use of a ‘legal high’, such as mephedrone, is a new phenomenon but mephedrone may be merely the first of many designer drugs that market themselves as ‘legal highs’ about which we know little initially in terms of their lethality and other harms.
The Table below sets out some scenarios to conjure with. If mephedrone’s lethality were considerably lower than for cocaine and its potential considerable to avert users from cocaine, then even high-prevalent use of mephedrone could limit DRDs in practice.
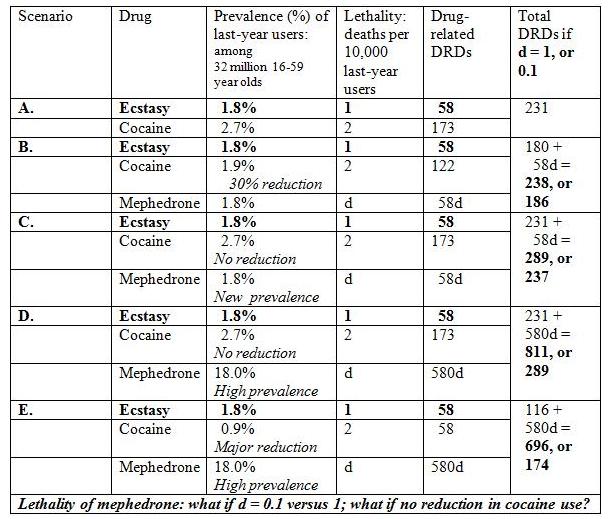
Testing all DRDs in 2010 for mephedrone: If mephedrone-related DRDs occurred at a rate of 0.1 per 10,000 users and mephedrone-prevalence was two-thirds that of cocaine, then we’d expect about 6 mephedrone-related deaths in 2010.
But if mephedrone-related deaths were 1 per 10,000 last year users (as for ecstasy), then we’d expect 58 (nearly 60) mephedrone-related DRDs and so about 20 (approximate 95% CI: 12 to 31) in just 4 months. That is, about one per week . . . Uniform toxicological testing of all DRDs for mephedrone in March to June 2010 should be a priority – not least if we want well-evidenced decision-making.
When UK is prepared to £6 millions pounds per annum to check up the expenses of members of both Houses of Parliament, can we not suggest a 5% efficiency saving to afford the £300,000 needed to learn rigorously about the age-specific use and lethality of mephedrone?
* BIRD SM, Lynskey M, English C, Donnelly J, Michael M, Treble R. Revisiting British Army Drug Testing, 2003-07: test thresholds, efficient targeting, and underlying trends. Journal of Royal United Services Institute (RUSI) 2008; 153: 16 - 23.

christopher crossman (not verified) wrote,
Wed, 03/03/2010 - 20:34
you mentioned British Crime Survey figures. Some years ago I did some field interviewing for a big MR firm (Milward Brown, I think) calling on pre-selected urban households in the Wirral area, asking respondents their experience of of local crime. The client was the Home Office British Crime Survey.
In the briefing notes we were told to cut short any interview or ignore the incidents in which the crime experience related had not been actually reported to the Police. Of course there were possible good reasons for this, not least to obviate duplicated reports by more than one person and, presumably, to make the results comparable with the Police Forces's own statistics. However it always struck me that the policy also necessarily-meant that a large proportion of actual but enreported crime went unquantified.
Furthermore in areas where assault, intimidation, theft and deception were most rife, and people in those area most likely to inured and resigned to such everyday incidents, or hostile or cynical towards the Police, this practise necessarily resulted in a misleading and inaccurate picture of the true situation. so the BCS cannot represent numbers or changes or trends of incidence of crime - only changes or trends in the reporting of crime -which is much more manageable. CC
NV (not verified) wrote,
Mon, 31/05/2010 - 10:03
It is a very interesting article. Here is some more info about it : http://www.videorolls.com/watch/The-Truth-About-Mephedrone
Samuel (not verified) wrote,
Tue, 24/08/2010 - 11:23
Great info about Mephedrone.I have bookmarked your posting for future reference.Chicago mover
Emma Goldman (not verified) wrote,
Sat, 30/10/2010 - 03:04
The only way to speed up legislation to outlaw the drug is for the EU agency, European Monitoring Centre for Drugs and Drug Addiction to produce its own report on the health risks associated with using the drug. This could then be used as a blueprint to help speed the process up once the ACMD group has been rebuilt. Vetement Grossesse