How lethal is mephedrone? Dealing with registration delays
Mephedrone will soon join the list of banned drugs, as a result of the advice of the Advisory Council on the Misuse of Drugs to classify it as a Class B drug alongside cannabis and amphetamines. Effective legislation will come into force tomorrow.
Several deaths have been linked to mephedrone use, but we lack epidemiological evidence by which to determine whether mephedrone is more, or less, lethal than cocaine. If it is less lethal, and if mephedrone has been commonly used as an alternative to cocaine/ecstasy, we might begin to see a decline in cocaine-related deaths. What do the statistics tell us?
During the monitoring of the swine flu epidemic, child deaths from respiratory causes were an issue of particular interest. Parliamentary attempts to elicit early data on respiratory deaths in children aged 1-14 years failed. Data for previous years were provided, however, as a relevant backdrop against which to compare the 2009 deaths when they are officially reported.
Mephedrone is another epidemic, believed to have started in 2008. There is some evidence that young people may have taken it up as alternative, or adjunct, to cocaine and ecstasy. In the British Army, for example, soldiers’ cocaine positive rate in compulsory drug tests nose-dived from 5.2 per 1,000 tests (95% CI: 4.7 to 5.8) in the first three quarters of 2008 to 3.5 in the fourth quarter. Soldiers’ cocaine-positive rate was down to 1.9 per 1,000 tests by the fourth quarter of 2009.
It would be really instructive to apply the same logic to national figures for drugs-related deaths (DRDs) in England and Wales over the same period. In particular, has there been a fall in cocaine-related deaths (C-related deaths)?
Two complications arise. First, England and Wales reports DRDs by year/quarter of registration – not by year/quarter of death. For DRDs, the delay between quarter of death and quarter of registration may be six months or more because DRDs are subject to coroners’ inquiries. However, when tracking epidemics, it is quarter/year of actual death that matters.
Secondly, no information on DRD-registrations in 2009, some of which pertain to DRDs in 2008, will be available until after the annual data-freeze in May 2010 which enables official statistics on DRD-registrations in 2009 to be reported in the autumn of 2010.
Helpfully, and by request, the Office for National Statistics (ONS) has provided information on quarter/year of death against registration year for C-related DRDs in 2005 to 2007. These data are shown in Table 1, and allow us to estimate (crudely) that:
- 117/134 (87%) of C-related DRDs in Q1 of a given year were registered in the same year
- 126/160 (79%) of C-related DRDs in Q2 of a given year were registered in the same year
- 75/160 (47%) of C-related DRDs in Q3 of a given year were registeered in the same year
- 7/147 ( 5%) of C-related DRDs in Q4 of a given year were registered in the same year
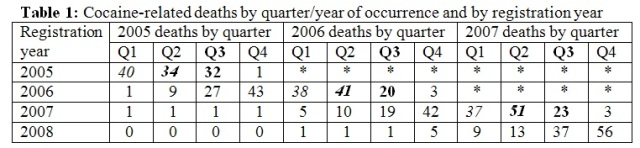
Footnote: Q3’s 75/160 = (32+20+23)/(32+27+1 + 20+19+1 + 23+37+?). For less crude estimators than above, we should really assume 1.6 for ? and so adopt, for example, 75/161.6 (46%) as estimator. For simplicity, both adjustments (i) and (ii) in Table 2 below are thus somewhat cruder than, strictly, they should be.
In the above estimates, we basically assume that registration delays have not altered throughout 2005-2007. Were we to rely only on the data for 2007 to estimate the adjustment factor for Q3, we should apply a proportion such as 23/60 (38%) or 23/61.6 (37%), not 75/160.
Registration delays are longer for DRDs, inevitably, because DRDs are subject to coroners’ inquiry. However, the extent of delay in such inquired-into deaths, as shown above, raises a serious question about whether a single data-freeze per annum is sufficient for the timely monitoring of epidemics. The question has poignancy because UK has confronted two major epidemics in 2009 with potentially lethal consequences for young people.
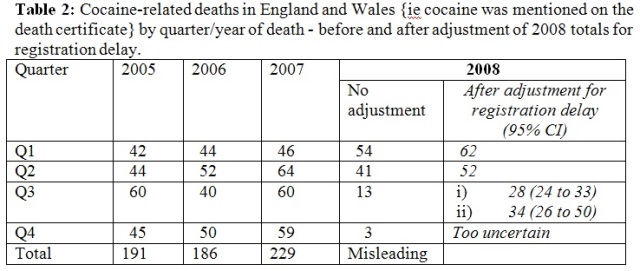
Table 2 illustrates how the above registration delays affect the quarterly totals for England and Wales of C-related DRDs for 2008. Quarterly totals have to be adjusted, as shown in the final column of Table 2, to compensate for late-registrations of C-related DRDs that actually occurred in Q3 of 2008. Adjustment is not even worth attempting for Q4 of 2008, about which we know altogether too little on the basis of the most recent data-freeze (in May 2009).
Across 2005-2007, the mean quarterly occurrence of C-related deaths in England and Wales has been 50.5. After adjustment i) for registration delay, we estimate that there may be around 28 C-related DRDs in Q3 of 2008 – an apparent decrease. But if registration delay had actually got worse from 2007 onwards, the resulting uncertainty about the alternative adjustment (ii) means that it would be premature to suggest that C-related DRDs had truly decreased in the third quarter of 2008.
In conclusion, no conclusion - except that the monitoring of epidemics requires that we track deaths by their quarter/month of occurrence, not by their quarter/month of registration. And, when registration delays are as extensive as for drug-related deaths, special measures may be needed, such as a 6-monthly data-freeze, to better inform public health decisions about new epidemics.
Sheila M. Bird writes as visiting professor, Department of Mathematics and Statistics, University of Strathclyde.

Anonymous (not verified) wrote,
Sun, 05/09/2010 - 05:06
I follow your logic. brilliant inference. I'm wondering what the corresponding stats are for Meph. It most certainly looks like deaths from Cocaine have gone down since the upsurge in popularity of Meph.
Do you know where Meph originated? I've read about the stimulant Khat and also that it's similar to an antidepressent which I immediately thought of when I read that it is a Seratonin Reuptake Inhibitor.
Thanks!