Drug tests in prison: how intelligently are they being used?
How smart have prisons in England and Wales been in using the information gained from mandatory drug testing? And which prisons have done better than others?
The data gathered by the mandatory testing programme - which includes both random and targeted tests - ought to be able to answer questions such as these, in order to improve the control of illicit drugs in prison. Thanks to MPs who have asked a series of parliamentary questions – and no thanks to the Ministry of Justice, which has been sparing in its release of data – we can attempt to answer this question.
At issue is: by how much does the intelligence available to prison officers improve their targeting of mandatory tests - over and above the detection rate achieved by random selection of whom to test and when? Mandatory tests are seen by many as a breach of prisoners’ human rights, and so they need to be justified by their efficacy in detecting drug-users, and in improving the choice of prisoners to be subjected to intelligence-driven targeted tests.
In this article I will use data from the two types of mandatory tests (random versus targeted) to compare two groups of prisons – those who carry out random mandatory drug tests (rMDTs) on 5 per cent of their inmates every month, and those that test a different per cent, usually higher and usually 10 per cent. The 10 per cent level used to be the norm, but now, sensibly, every year governors of larger prisons are allowed to elect for the 5 per cent level if they choose.
Smaller prisons do not have this option, because if they took it the number of tests would be too small. They are not allowed to deviate from 10 per cent rMDT unless they are big enough so that their annual total of rMDTs would be sufficient for precise estimation of the prison’s key performance indicator.
In July 2009, Andrew Pelling MP posed parliamentary questions on rMDT versus tMDT which were designed to compare how prisons’ index of suspicion for specific drugs had evolved over the period 2002/03 to 2008/09; and to contrast the performance of intelligence-led tMDT by prisons electing for, or against, 5 per cent rMDT.
The “index of suspicion” for illicit opiates is defined as: opiate positive rate in tMDTs/opiate positive rate in rMDTs. Statistics on rMDTs refer to the number of tests, not to the number of individuals tested. The difference is more critical for tMDTs as repeat testing of individuals who have ever-tested positive for illicit drugs is a possible strategy for selecting inmates for serial testing in tMDT.
Because heroin stays in the urine for only two to three days, rMDT detects only one in about 3.5 inside-users of heroin. The same caveat does not apply to tMDT because on-suspicion testing is likely to occur soon after the prisoner’s inside-use of heroin. Thus, the opiate positive rate in tMDT can be up to 3.5 times greater than in rMDT just by ensuring recency of inside-use when tMDT is invoked. This type of ‘timing-uplift’ does not enhance tMDT’s yield of cannabis positives to the same extent because cannabis stays in the urine anyway for up to two weeks.
In summary, the ratio of positive rates in tMDT versus rMDT should be higher for opiates than for cannabis because naturally-uplifted by a ‘timing bonus’. Opiate positive ratios in excess of 3.5 are evidence of intelligence-led targeting beyond just timing.
Table 1 shows that the number of prisons electing for 5 per cent rMDT increased from 72 in 2002/03 to 90 in 2008/09. If prisons in Table 2 which elected against 5 per cent rMDT can be assumed to have operated 10 per cent rMDT, then the average prison population in England and Wales may be assumed as {20 * 30,094 + 10 * 24,419}/12 = 70,506 in 2002/03, rising by 18 per cent to {20 * 40,195 + 10 * 19,360}/12 = 83,125 in 2008/09.
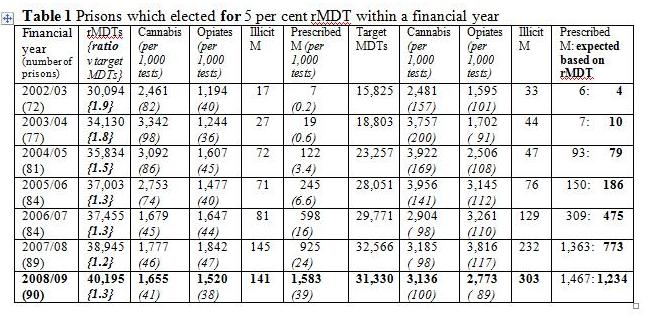
Year-on-year, the opiate positive rate in rMDT (and likewise for the cannabis positive rate) was higher in prisons which elected for 5 per cent rMDT (compare Tables 1 and 2) which will have tended to be larger establishments. By 2007/08 and 2008/09, prescribed methadone was being offered to 2.4 per cent and around 4.0 per cent of inmates in both sets of prisons so that prisons’ Integrated Drug treatment System (IDTS) clearly included smaller as well as larger establishments.

If prison budgets for mandatory drugs testing are limited, or indeed capped, it is unsurprising that the ratio of rMDTs versus tMDTs is lower in establishments which are able to elect for 5per cent rMDT and so devote more test-resources to tMDT. Thus, Table 1 shows that, in 2008/09 for example, prisons which elected for 5 per cent rMDTs performed 40,195 rMDTs but 31,330 tMDTs, a test ratio of 1.3 whereas prisons which elected against 5% rMDT did 19,360 rMDTs but only 6,636 tMDTs which gave them a test ratio of 2.9, see Table 2.
How wisely did the (mainly smaller) prisons that elected against5 per cent rMDT deploy their relatively low number of tMDTs?
Index of suspicion for specific drugs: Table 3 shows that, year-on-year, the ratio of drug-specific positives in tMDT versus rMDT was higher – both for cannabis positives (6 out of 7 yearly comparisons) and for opiates positives (all 7 yearly comparisons) – in prisons which elected against5 per cent rMDT.
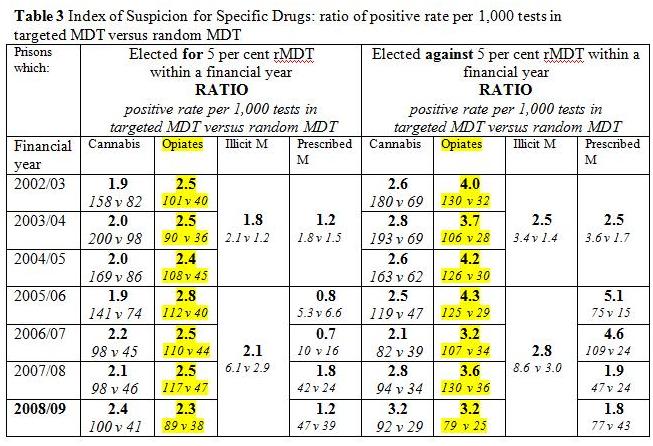
Only in prisons which elected against 5 per cent rMDT did the ratio of opiate positives in tMDT versus rMDT approach or exceed 3.5. Intelligence-led deployment of tMDTs has been superior in the set of typically smaller prisons which elected against 5 per cent rMDT. However, security rating and functionality, as well as size may differ between establishments which elect for rather than against5 per cent rMDT.
As expected, the timing-uplift for opiates has contributed to the index of suspicion being uniformly higher, year-on-year and within each set of prisons, for opiates than for cannabis. This relates to the substantial under-detection by rMDT of inside-users of opiates because heroin stays in the urine for only two to three days, and determination within rMDT not only of whom to test but also when to test whereas tMDT can optimize when a targeted individual is tested in relation to their inside-use of heroin.
Finally, it appears that the prisons which elected against5 per cent rMDT preferentially imposed tMDT on inmates who had been prescribed methadone but that such targeting, in 2005/06+2006/07 especially (see ratios for prescribed methadone of 5.1 and 4.6), did not seem to yield any specific pay-off in enhanced detection of opiate positives so that, quite sensibly, by 2007/08 this sort of targeting had been relaxed so that the prescribed methadone test ratio dropped back to under 2.0.
Conclusions: Insightful analysis of positive rates for specific drugs in tMDT versus rMDT suggests a different, and more successful, profile for intelligence-led tMDT in prisons which elected against5 per cent rMDT. Relatively speaking, they deploy fewer tMDTs to greater effect. Neither set of prisons – those which elected for, or against, 5 per cent rMDT – shows a clear trend for drug-specific indices of suspicion to have improved over the period from 2002/03 to 2008/09.
